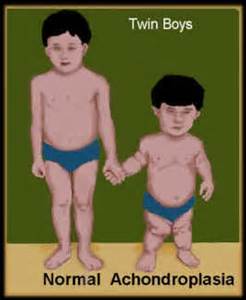
Achondroplasia
It is a disorder of the bone growth that causes disproportionate dwarfism. Dwarfism is is a condition of short stature as an adult; humans with achondroplasia are short in stature with a short limbs and normal sized torso.
Causes: In achondroplasia, a lot of the cartilage doesn’t convert into bone; this is caused due to mutations in the FGFR3 gene. This gene instructs the body to make proteins necessary for bone growth and maintenance, an abnormally large, prominent forehead short arms and legs, short fingers, apnea, spinal stenosis, difficulty in bending elbows.
Pathophysiology: This disorder is caused by mutations in the fibroblast growth factor receptor-3 (FGFR3) gene. FGFR3 has been mapped to the short arm of chromosome 4, the 2 mutations, G1138A and G1138C, cause increased function of the FGFR3 gene. These mutations causes decreased endochondral ossification, decreased cellular hypertrophy, decreased cartilage matrix production, and inhibited proliferation of chondrocytes in growth plate cartilage.
Diagnosis:
Treatment:
Medical Care: Closely monitor Weight, height, and body growth in patients with achondroplasia using achondroplasia-specific growth charts, measure and record the upper-to-lower segment ratio.
Somatropin (recombinant human growth hormone [HGH]): To foster linear growth HGH therapy should be administered. It effectively increases the bone growth rate, especially for the first year of use. To achieve maximum benefit, this therapy is recommended at the age of 1-6 years.
NSAIDs (non-steroidal anti-inflammatory drugs): To decrease the pain and inflammation for patients with degenerative joint disease these drugs are preferred.
Medications:
Genotropin: 0.16 mg/kg to 0.24 mg/kg per week; divided into equal 6-7 SC doses/week
Norditropin: 0.024-0.034 mg/kg/day SC 6-7 days/week
Humatrope: 0.026-0.043 mg/kg/day (0.18 mg/kg/week - 0.3 mg/kg/week) SC divided into 6-7 equal doses/week SC doses)
Prepuberty: 0.3 mg/kg/week SC weekly divided into equal daily doses
Postpuberty: Not to exceed 0.7 mg/kg/week divided into equal daily doses
Omnitrope: 0.16-0.24 mg/kg/week SC divided into 6-7 doses/week
Saizen: 0.18 mg/kg/wek SC/IM divided into equal doses
Zomacton: Up to 0.1 mg/kg SC 3x/week
Genotropin, Omnitrope: 0.48 mg/kg/week SC divided into equal doses 6-7 days/week
Humatrope: 0.47 mg/kg/week SC divided into equal doses 6-7 days/week
Norditropin: Not to exceed 0.067 mg/kg/day SC
Norditropin: Not to exceed 0.066 mg/kg/week SC
Nutropin, Nutropin AQ: Not to exceed 0.35 mg/kg/week divided into equal doses for 6-7 days; continue until time of renal transplantation
Genotropin: 0.24 mg/kg/week SC divided into equal doses for 6-7 daily injection
Omnitrope: 0.24 mg/kg/week SC divided into 6-7 daily injections
Norditropin: Not to exceed 0.067 mg/kg/day SC
Genotropin: 0.33 mg/kg/week SC divided into 6-7 days/week
Omnitrope: 0.33 mg/kg/week SC divided into 6-7 daily injections/week
Humatrope: Not to exceed 0.054 mg/kg/day SC (0.375 mg/kg/week divided into 6-7 days/week)
Nutropin and Nutropin AQ: Not to exceed 0.375 mg/kg/week SC divided into 3-7 days/week
Achondroplasia, dwarfism, birth defects